Quick Summary: Key Takeaways
- Generic errors often stem from physical differences (color, shape) and look-alike/sound-alike names.
- Tech tools like BCMA and CPOE can cut medication errors by 50% to 55%.
- Patient counseling for first-fill generics catches roughly 15-20% of potential misunderstandings.
- Medication reconciliation is the most effective manual way to find discrepancies during transitions of care.
Why Generics Create Unique Error Risks
The core of the problem is that Generic Medications is a category of drugs created to be bioequivalent to brand-name products, meaning they have the same active ingredient but may differ in inactive fillers, color, and shape. While the FDA requires an absorption range of 80-125% to prove bioequivalence, the physical appearance varies wildly between manufacturers. This is where the danger kicks in.
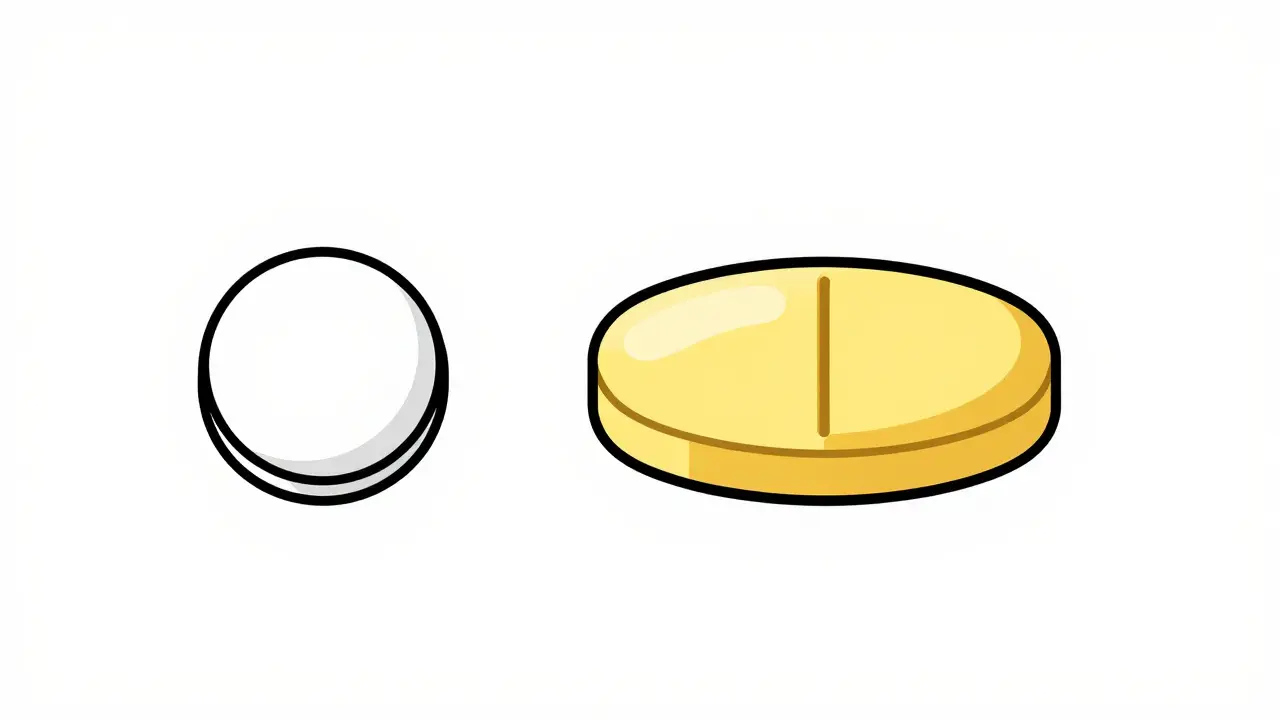
Imagine a patient who has been taking a generic statin that is a small white round pill. Suddenly, the pharmacy switches to a different generic manufacturer, and the pill is now a large yellow oval. The patient may panic, thinking they have the wrong medication, or worse, they might double-dose because they don't recognize the new pill. These "dispensing form" issues are a major driver of clinical errors. In fact, research shows that about 14.4% of clinical errors in community pharmacies involve the dispensing form.
Then there is the "look-alike, sound-alike" (LASA) problem. Generic chemical names are often complex and similar, making it incredibly easy for a tired technician or pharmacist to grab the wrong bottle from the shelf. When you combine these naming issues with the pressure of high-volume retail settings, the margin for error shrinks.
The Heavy Hitters of Error Prevention Technology
We can't rely on human memory alone. Technology acts as the primary safety net, though no single software is a magic bullet. The most effective systems focus on removing the manual "guesswork" from the equation.
First, there is CPOE (Computerized Physician Order Entry). By eliminating handwritten prescriptions, CPOE reduces errors by about 55% in hospitals and 48% in primary care. It stops the "guessing game" of deciphering a doctor's scrawl, which is where many generic substitution mistakes begin.
Then we have BCMA (Bar Code Medication Administration). This is the process of scanning the medication and the patient's wristband to ensure a match. Implementing BCMA has been shown to reduce potential adverse drug events by 50%. It's the ultimate "sanity check" before the drug ever reaches the patient.
Finally, CDSS (Clinical Decision Support Systems) provide real-time alerts. These systems can flag if a generic substitution is inappropriate for a specific patient or if there's a therapeutic duplication. However, a word of caution: too many "stop alerts" can lead to alert fatigue, where pharmacists start clicking "dismiss" without reading the warning, effectively neutralizing the tool.
| Technology | Estimated Error Reduction | Primary Strength | Main Weakness |
|---|---|---|---|
| CPOE | 48% - 55% | Eliminates handwriting errors | Initial implementation time |
| BCMA | 50% | Verifies correct drug/patient | Requires hardware at point of care |
| CDSS | Varies (High) | Flags drug-drug interactions | Alert fatigue |

The Human Element: Manual Safeguards and Protocols
Even with the best software, the human touch is where the final catch happens. The most reliable manual framework is the "8 R's of medication safety": right patient, drug, time, dose, route, documentation, reason, and response. Training a team on this takes about 8-12 hours, but it creates a mental checklist that catches errors technology might miss.
Another critical step is Medication Reconciliation, which is the process of creating the most accurate list possible of all medications a patient is taking and comparing that list against the physician's orders. This is especially vital when a patient is discharged from a hospital. Pharmacists spending 15-20 minutes on a thorough review can find an average of 2.3 discrepancies per patient. Often, these are generic brands that were changed during a hospital stay without the patient's knowledge.
Don't underestimate the power of the 5-minute conversation. Mandatory counseling for first-fill medications-especially generics-is a massive safeguard. When a pharmacist explains, "This pill is blue, but your previous one was white, and they do the exact same thing," it prevents patient panic and potential misuse. Data suggests that 15-20% of counseling sessions catch potential misunderstandings about generic substitutions.
Common Pitfalls and How to Correct Them
Even the most experienced pharmacists hit roadblocks. One of the biggest is outdated drug information. About 42% of pharmacists report that their reference systems have outdated formulation details. If you're relying on a database from three years ago, you might not know that a generic manufacturer changed their excipients, which could trigger an allergic reaction in a sensitive patient.
To correct this, you need a strategy for information freshness. Using updated digital assistants like Epocrates or maintaining a current subscription to 'Drug Facts and Comparisons' is essential. It’s a small investment (around $150-$300 annually) that prevents a catastrophic error.
Another common pitfall is the "communication gap" between the prescriber and the pharmacy. Many doctors aren't aware of the specific manufacturer formulations being used in the community. If a patient has a known adverse reaction to a specific filler in a generic, the pharmacist must document this and communicate it back to the provider to ensure a "dispense as written" (DAW) order is placed for the brand name or a different generic.

Steps to Build a Safer Generic Dispensing Workflow
- Audit Your Inventory: Identify LASA (look-alike, sound-alike) generics and physically separate them on the shelf. Use "Tall Man" lettering (e.g., HYDROCORTISONE vs. HYDRALAZINE) on bin labels.
- Implement a Double-Check System: Ensure that the person who pulls the generic from the shelf is not the same person who performs the final verification.
- Update Your Database: Move away from static spreadsheets and use a real-time drug information system that flags manufacturer changes.
- Prioritize First-Fill Counseling: Make it a non-negotiable rule that any new generic substitution requires a 3-minute patient briefing on the drug's appearance and purpose.
- Track Your "Near Misses": Don't just track the errors that reached the patient. Keep a log of the errors you caught. This reveals patterns-like a specific generic that is always mispicked-allowing you to fix the root cause.
Are generic drugs less effective than brand names, leading to more errors?
Generally, no. The FDA requires generics to be bioequivalent, meaning they deliver the same amount of active ingredient to the bloodstream (within an 80-125% range). The "errors" associated with generics are usually operational-like confusing a yellow pill for a white one-rather than a failure of the drug's chemical efficacy.
How do I handle a patient who refuses a generic substitution?
First, listen to their concerns. If they've had a bad reaction to a generic in the past, it might be due to an inactive ingredient (excipient). In these cases, contact the prescriber to request a "Dispense as Written" (DAW) order for the brand-name version to ensure patient safety and adherence.
What is the most common cause of generic-related dispensing errors?
The most common causes are administrative (like incorrect data entry) and clinical (like dosage or strength discrepancies). Specifically for generics, the "dispensing form"-the physical look of the pill-is a primary source of confusion for both pharmacists and patients.
Can AI really help prevent generic medication errors?
Yes. New AI-powered clinical decision support systems can now predict adverse reactions based on a patient's unique pharmacogenomics. Pilot programs have shown a 22% additional reduction in errors beyond what standard software can achieve by tailoring generic choices to the individual patient.
How often should pharmacy staff be retrained on the "8 R's"?
While initial training takes 8-12 hours, a quarterly refresher or "safety huddle" is recommended. This keeps the framework top-of-mind and allows the team to discuss recent near-misses and update their protocols.
Next Steps for Different Pharmacy Settings
For Retail Pharmacy Owners: Focus on the infrastructure. If you haven't adopted BCMA or a modern CDSS, the ROI is clear: a 50% reduction in adverse events is worth the $25,000-$75,000 investment. Start by auditing your most common generic errors to see where the gaps are.
For Staff Pharmacists: Focus on the patient interaction. Implement a strict first-fill counseling protocol. Even if the pharmacy is slammed, those three minutes spent describing the generic pill can prevent a phone call (or a medical emergency) tomorrow.
For Hospital Pharmacy Managers: Prioritize the discharge process. Medication reconciliation at the point of transition is where most generic discrepancies are found. Ensure your pharmacists have dedicated time (15-20 minutes per patient) to conduct a proper review before the patient leaves the building.


Maggie Graziano
pharma companies just swap colors to keep us confused dont trust the generic labels
ira fitriani
This is such a vital reminder for all of us! 🌟 It's all about that human connection and making sure the patient feels seen and safe. Let's keep pushing for better care everywhere! 💪✨
Randall Barker
The fundamental failure here isn't the technology, but the moral bankruptcy of a system that prioritizes profit margins over the sanctity of human life. We treat medication like a commodity and then act shocked when the 'bioequivalent' shell game leads to disaster. It's a systemic erosion of professional ethics where the pharmacist is reduced to a glorified pill-counter in a corporate machine. If we cannot guarantee the absolute integrity of the substance being ingested, we have failed the most basic philosophical contract between healer and patient. The reliance on BCMA is just a band-aid on a gaping wound of corporate greed. We are sacrificing quality for the sake of a spreadsheet, and the cost is measured in human suffering. It is an absolute travesty that we even have to discuss 'near-misses' as a metric for success rather than demanding a flawless system. The only real solution is a complete overhaul of the pharmaceutical distribution model to remove the incentive for cheap, interchangeable generics that gamble with patient psychology. Until then, we are just managing the fallout of a broken ideology. Truly pathetic.
Michael Lewis
Spot on with the importance of the double-check system. No matter how fast the pace is, taking that extra second to verify prevents a lifetime of regret. Keep it up everyone!
Anna BB
It's interesting to think about how a simple change in pill color can affect a person's mental state... the psychology of healing is so complex!!! I wonder if we focus too much on the tech and not enough on the peace of mind??
Joshua Nicholson
eh just use the scanner and it's fine lol