Handling chemotherapy isn’t just about giving a patient a drug. It’s about protecting the nurse, the caregiver, the pharmacist, and even the family member who might clean up a spill. One mistake - a torn glove, a skipped check, a spilled vial - can expose someone to a toxin that doesn’t just kill cancer cells. It can damage bone marrow, harm reproductive organs, and increase cancer risk in healthy people. The stakes are that high.
Why Chemotherapy Is Different From Other Medications
Most drugs are designed to be safe for healthy people to handle. Chemotherapy drugs aren’t. They’re made to kill fast-growing cells. That’s great for tumors. Not so great for skin, hair follicles, or a developing fetus. Even tiny amounts - a drop on the skin, a breath of aerosol during mixing - can cause long-term harm. That’s why the rules changed.
In 2024, the American Society of Clinical Oncology (ASCO) and the Oncology Nursing Society (ONS) updated their standards to reflect today’s reality: chemotherapy isn’t just traditional pills and IVs anymore. It includes targeted therapies, immunotherapies, and antibody-drug conjugates. All of them carry the same risk. That’s why the term now is antineoplastic therapy. The name change wasn’t just for show. It meant the safety rules had to cover everything, not just the old-school drugs.
The Four Pillars of Safe Administration
The 2024 ASCO/ONS standards break safety down into four non-negotiable areas. Skip one, and you’re risking lives.
- Safe Environment: Every treatment room needs engineering controls. That means closed-system transfer devices (CSTDs) for mixing and transferring drugs, negative-pressure ventilation in preparation areas, and spill kits within arm’s reach. No more pouring powders into beakers on an open counter. That’s a relic from the 1990s.
- Patient Consent and Education: Before the first dose, the patient must know exactly what they’re getting - drug name, dose, side effects, duration, and goals. This isn’t a formality. It’s a legal and ethical requirement. If the patient doesn’t understand, the treatment shouldn’t start.
- Ordering, Preparing, and Administering: This is where most errors happen. The old two-check system is gone. Now, there’s a mandatory fourth verification - done at the bedside, right before the IV starts. Two licensed staff members must confirm the patient’s name, date of birth, drug, dose, and route. And they do it together, in front of the patient. No exceptions. This step alone cut patient identification errors by 18% in the 2022 NCCN database.
- Monitoring During and After: Some drugs, especially immunotherapies, can trigger cytokine release syndrome (CRS). That’s when the immune system goes into overdrive, causing fever, low blood pressure, and organ failure. Mortality can hit 15% if not treated fast. Now, every facility must have antidotes like tocilizumab on hand and a written protocol for how to respond. No more guessing.
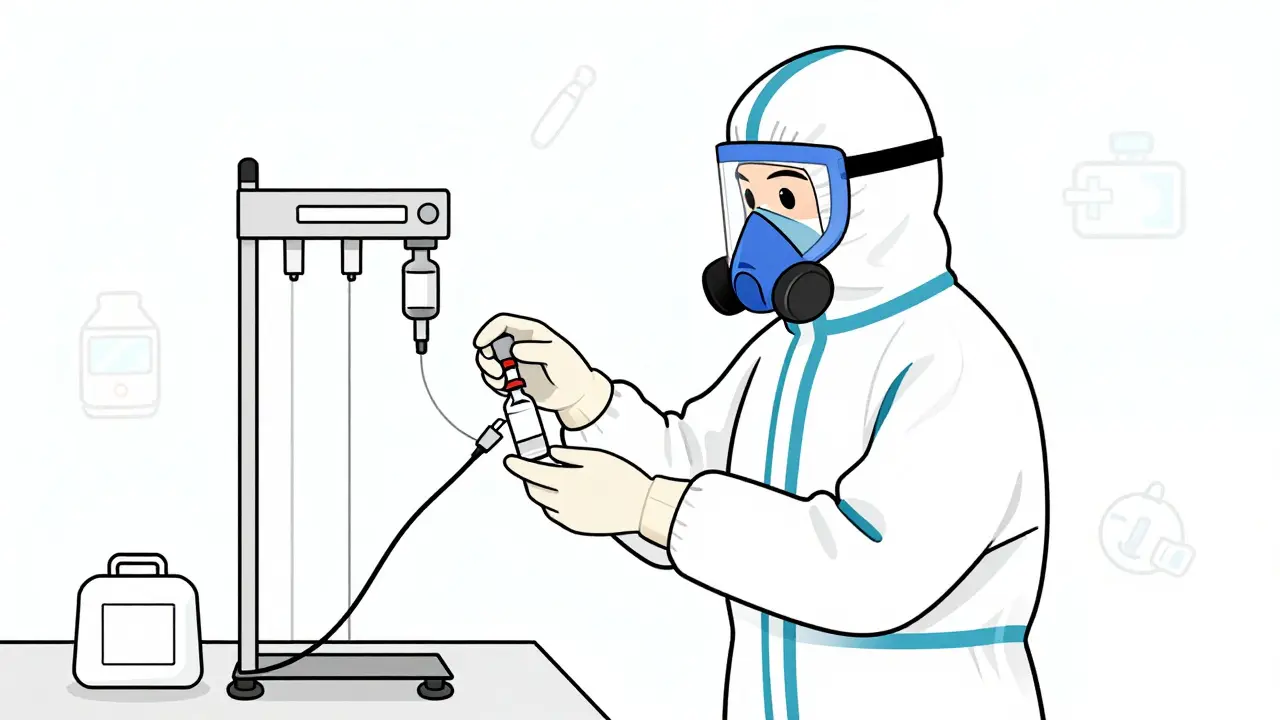
Personal Protective Equipment (PPE) - It’s Not Optional
Wearing gloves? Good. Wearing the right gloves? That’s the difference between safety and exposure.
NIOSH and USP <800> require chemotherapy-tested double gloves. Not just any gloves. They must be tested for permeation by at least six chemotherapy drugs, including high-risk ones like carmustine and thiotepa. Single gloves? They fail within minutes. Double gloves? They can last 30 minutes or more. And they must be changed every 30 minutes - or immediately if torn.
That’s not all. You need an impermeable gown - not a lab coat. Eye protection if splashing is possible. And if you’re mixing drugs in a room without proper ventilation, you need a respirator. N95s won’t cut it. You need a P100 or powered air-purifying respirator (PAPR) for aerosol-generating procedures.
And here’s the part no one talks about: everything you wear during chemo handling is contaminated. Even if it looks clean. Studies from 1992 to today show that outer gloves transfer drugs to skin, surfaces, and even your phone. So you don’t take your gown home. You don’t reuse your gloves. You treat them like radioactive waste.

Home Chemotherapy - The Hidden Risk
More than 30% of cancer patients now get chemo at home. That’s a huge shift. But the safety standards? They were written for hospitals. Home care is a gap.
The American Cancer Society found that 22% of home incidents involve improper disposal of chemo waste - like syringes, IV bags, or even soiled tissues. Another 17% involve no plan for spills. Patients are told to store drugs in child-proof containers. But what if they forget? What if they don’t have a lockbox? What if they’re too sick to follow instructions?
Facilities that use the ASCO-developed Chemotherapy Safety at Home toolkit see a 41% drop in caregiver concerns. That toolkit includes color-coded disposal bags, step-by-step spill videos, and a 24/7 hotline. But not every clinic offers it. And in rural areas, where resources are thin, home chemo is often handed out with a pamphlet and a prayer.
Who Pays for Safety? The Real Cost
Safe chemo administration isn’t cheap. A medium-sized clinic needs $22,000-$35,000 to upgrade ventilation and install CSTDs. Another $8,500-$12,000 for staff training. Then there’s the annual cost: $4,200-$6,800 just for gloves, gowns, and hazardous waste disposal.
And the EHR? Most electronic systems weren’t built for four-step verification. Facilities report spending $15,000-$40,000 to customize their software. That’s a huge barrier for small practices. Dr. Sarah Temkin from UVA Health points out that 43% of rural clinics can’t afford full CSTD implementation. That’s not a policy gap - it’s a justice gap. Patients in wealthy cities get safer care than those in small towns.
But here’s the flip side: facilities that do it right see 63% fewer medication errors and 78% fewer staff exposures. OSHA fined 142 facilities in 2022 for chemo safety violations. The average fine? $14,250. Paying for safety upfront saves money - and lives.
What’s Next? AI, Certification, and New Drugs
The future of chemo safety is here - and it’s digital. By Q3 2024, 12 NCI-designated cancer centers are testing AI-powered verification systems. These tools scan patient wristbands, drug labels, and IV bags, then cross-check everything against the electronic order. If something’s off, it stops the process. No human error. No skipped step.
By 2026, a national certification for chemo administration staff is expected. Think of it like a license to handle hazardous drugs. No certification? No handling.
And new drugs? Bispecific antibodies and antibody-drug conjugates are coming fast. They’re more powerful. But they also leak more easily. Their handling rules aren’t fully written yet. That’s why the ASCO standards are called “living documents.” They change every 5-7 years - because the drugs do.
What Nurses and Caregivers Really Say
On Reddit, nurse ChemoRN2020 wrote: “The fourth verification adds 7-10 minutes per patient. We’re already swamped. And our error rate hasn’t dropped.” That’s real. Staffing shortages make every extra step feel like a burden.
But 78% of nurses in a 2022 survey said their confidence jumped after full implementation. Why? Because they finally felt protected. Because they knew they had a system, not just a checklist.
And caregivers? Sixty-five percent feel unprepared. But those who got the toolkit? They slept better. They knew what to do if the bag leaked. They knew where to call. That’s not just safety - that’s peace of mind.
Do I need special gloves for chemotherapy handling?
Yes. You need chemotherapy-tested double gloves that meet NIOSH and USP <800> standards. Regular exam gloves are not enough - they can break down within minutes when exposed to drugs like carmustine or thiotepa. Gloves must be changed every 30 minutes or immediately if torn. Double gloving reduces skin exposure by over 90%.
What’s the fourth verification step in chemotherapy administration?
The fourth verification is a mandatory bedside check performed right before the drug is given. Two licensed staff members must confirm the patient’s full name, date of birth, drug name, dose, route, and time - all while the patient is present. This step was added in 2024 to prevent fatal misidentification errors, which caused 18% of chemotherapy-related adverse events in 2022.
Can I handle chemotherapy drugs at home without training?
No. Even if you’re a caregiver, you must be trained. Home chemo requires knowing how to store drugs safely, manage spills, dispose of sharps and bodily fluids, and recognize signs of adverse reactions. The American Cancer Society reports that 65% of home caregivers feel unprepared. Facilities that provide the ASCO Chemotherapy Safety at Home toolkit reduce these concerns by 41%.
What should I do if a chemotherapy spill happens?
Never clean a chemo spill with paper towels or a regular mop. Use a dedicated chemotherapy spill kit, which includes impermeable gloves, goggles, absorbent pads, and a biohazard bag. Evacuate the area, put on PPE, contain the spill, then absorb and dispose of everything as hazardous waste. Wash the surface with detergent and water afterward. Always report the spill - even if you think it was small.
Are oncology nurses at risk from long-term chemotherapy exposure?
Yes. Studies show nurses who handle chemo drugs have higher rates of miscarriage, infertility, and certain cancers. But exposure drops by 78% when full safety protocols are followed. Only 41% of exposed nurses report incidents because they fear retaliation. Facilities with formal exposure protocols and anonymous reporting see higher compliance and fewer long-term health effects.
Why are closed-system transfer devices (CSTDs) so important?
CSTDs prevent hazardous drugs from escaping into the air during mixing or transfer. They’re like sealed ports that allow fluid to move without releasing vapors or aerosols. Without them, even a small splash or evaporation can expose staff. The European Society for Medical Oncology (ESMO) considers CSTDs essential. In the U.S., 92% of accredited cancer programs now use them - up from 64% in 2016.
What happens if a facility doesn’t follow chemotherapy safety standards?
OSHA can issue citations with fines averaging $14,250 per violation. In 2022, 142 facilities were cited for hazardous drug handling. Beyond fines, non-compliance puts staff and patients at risk. The National Comprehensive Cancer Network (NCCN) will require proof of safety protocol adherence for facility accreditation starting January 2025. No compliance = no accreditation.
Final Thought: Safety Isn’t a Checklist - It’s a Culture
Chemotherapy safety isn’t about following rules because someone told you to. It’s about knowing that the person next to you - the nurse, the pharmacist, the caregiver - could be poisoned by a drop of drug they didn’t see. It’s about recognizing that the same drug that saves a life can end another if handled carelessly.
The tools exist. The standards are clear. The cost of doing it right is high - but the cost of doing it wrong is measured in lives. Every glove changed, every verification done, every spill kit stocked - it adds up. Not just to compliance. To care.



Margaret Khaemba
I’ve been a nurse for 12 years and I still get nervous every time I prep chemo. Not because I’m scared of the drug - I know the protocols - but because one slip-up can haunt you for life. I once saw a rookie forget to double-glove. Didn’t even realize it until her wrist was red the next day. We all mess up. But the system? It’s got to catch us before we hurt someone.
That fourth verification? Yeah, it adds time. But I’d rather be late than lethal. My patient last week said, ‘You’re checking again? I thought we already did.’ I smiled and said, ‘Yeah, but this time I’m looking you in the eye.’ He nodded. That’s the moment it stops being a checklist and starts being care.
And home chemo? My cousin got it at home. They gave her a pamphlet and a box of gloves. No video. No hotline. She spilled a bag and wiped it with a paper towel. I almost threw up reading her text. We need better. Like, now.
Why do we still use paper charts in some places? It’s 2024. We have AI that can scan barcodes faster than a human blink. Why aren’t we using it everywhere? It’s not about money - it’s about will.
I’m tired of hearing ‘we can’t afford it.’ What’s the cost of a nurse getting infertility because we cut corners? What’s the cost of a kid breathing in chemo dust from their mom’s coat? We’re not saving money. We’re stealing futures.
And don’t get me started on the rural clinics. My sister lives in West Virginia. She gets her treatment in a building that still uses the same gloves from 2010. No CSTDs. No negative pressure. Just prayers and duct tape. That’s not healthcare. That’s gambling with lives.
But hey - at least we’re talking about it. That’s something.
Still… I wish more people outside this field knew what we deal with every day. We’re not heroes. We’re just people trying not to kill the people we’re trying to save.
Daphne Mallari - Tolentino
It is, regrettably, a matter of profound disquiet that the medical establishment continues to treat chemotherapeutic safety as a discretionary protocol rather than an absolute bioethical imperative. The adoption of closed-system transfer devices, for instance, is not merely prudent - it is non-negotiable in the context of occupational health jurisprudence. The failure to enforce universal compliance constitutes a breach of the duty of care owed to all healthcare personnel, and I find it morally indefensible that such measures remain optional in any jurisdiction.
Furthermore, the notion that cost should dictate the standard of protection is not only archaic but dangerously misguided. The economic burden of occupational exposure - in terms of litigation, lost labor, and long-term morbidity - far exceeds the capital outlay required for proper infrastructure. One need only consult the OSHA penalty records to discern the fiscal folly of negligence.
It is imperative that accreditation bodies, including NCCN, enforce compliance with zero tolerance. No exceptions. No waivers. No rural exemptions. Safety is not a privilege reserved for urban centers. It is a human right.
And to those who lament the added time of the fourth verification: perhaps the issue is not the protocol, but the systemic under-resourcing that renders even the most basic safeguards burdensome. Fix the staffing crisis. Then we can discuss efficiency.
Neil Ellis
Man, I used to think chemo was just fancy poison for bad cells. Then I watched my aunt go through it - and saw the nurses in their full gear, like astronauts prepping for Mars. No joke. They look like they’re defusing bombs.
And the gloves? I thought gloves were gloves. Turns out, if you use the wrong kind, you might as well be licking the drug off your skin. Wild.
That fourth check? Sounds like a pain in the butt, but I get it. I’ve seen people grab the wrong pill bottle at the pharmacy. Imagine if that was chemo. One wrong dose and boom - someone’s life is over. No second chances.
And home chemo? My cousin’s mom got it at home. They gave her a Ziploc bag for disposal. A ZIPLOC. I almost cried. No wonder people are scared. We treat this like it’s just another prescription, but it’s not. It’s a live grenade wrapped in a syringe.
But hey - the AI thing? That’s next-level. Imagine a robot double-checking your meds while you’re half-asleep. That’s the future. I’m all for it. Let the machines do the boring stuff so humans can focus on being human.
And to the nurses reading this? You’re the real MVPs. Seriously. I don’t say that enough.
Alec Amiri
Ugh. Another ‘chemo is dangerous’ article. Newsflash: everything’s dangerous. You breathe air? You’re gonna get cancer. You drink water? Cancer. You walk outside? Cancer.
Stop acting like chemo is some magic poison. It’s just medicine. If you’re too scared to handle it, go work at a bakery.
And that ‘fourth verification’? You’re telling me nurses can’t remember a patient’s name? Maybe they should get better training instead of adding 10 minutes to every shift.
Also, ‘CSTDs’? Sounds like a new iPhone. I’m sure it’s expensive. But guess what? Insurance won’t cover your ‘safety theater.’ Patients are already paying $50k for treatment. Now you want them to pay $30k more for gloves?
Wake up. This isn’t science. It’s fear-mongering dressed up as policy.
Rob Sims
Oh wow. Look who’s crying about gloves again. The nurses are tired? Boo hoo. You think I’m tired of watching my mom vomit for 10 hours straight after chemo? You think I’m tired of watching her lose her hair? You think I’m tired of lying to her when she asks if she’s gonna die?
But sure, let’s make the nurses’ job harder. Let’s add another check. Let’s make them spend 7 more minutes per patient. Meanwhile, my mom’s sitting there wondering why she’s still alive while the system wastes time on paperwork.
And home chemo? You’re telling me families are getting a pamphlet? That’s not negligence. That’s criminal. You know who’s to blame? The hospitals. They outsource the danger so they don’t have to pay for it.
And don’t even get me started on the ‘AI solution.’ Oh yeah, let’s replace nurses with robots. Because nothing says ‘compassionate care’ like a machine scanning your wristband.
This whole thing is a circus. And the clowns are wearing double gloves and calling it progress.
Lauren Wall
Double gloves. 30-minute changes. Spill kits. All mandatory. Yet rural clinics still use single gloves. That’s not a gap. That’s a death sentence.
And no one talks about the cost of silence. Nurses don’t report exposures because they’re scared of being labeled ‘difficult.’ So we’re flying blind.
Fix the culture. Not just the gear.
Kenji Gaerlan
why do they even use gloves if they still get exposed? i mean like, if the drug gets through the gloves, then what’s the point? just wear a hazmat suit and call it a day.
also why is everyone acting like this is new? my uncle got chemo in 1998 and they had the same rules. they just call it ‘antineoplastic’ now to sound fancy.
and the ai thing? lol. my cousin works at a hospital and their system crashes every time someone types ‘dox’ instead of ‘doxorubicin.’ so yeah, let’s trust robots to save us.
Akriti Jain
They’re lying. 😈 Chemo isn’t dangerous - it’s a cover-up. The real reason they’re pushing all these rules is because Big Pharma wants to make you think the drugs are too toxic to handle without their $200 gloves and $5000 machines. Meanwhile, they’re selling you the same poison for $100k a dose.
And that ‘AI verification’? It’s a tracking system. They’re logging every nurse’s move. Soon, you won’t be able to even change a glove without the algorithm flagging you for ‘non-compliance.’
They want you scared. Scared of the drug. Scared of the system. Scared of your own shadow.
And don’t get me started on the ‘24/7 hotline.’ That’s a trap. They’ll record your voice and use it to deny your workers’ comp claim later.
Wake up. This isn’t safety. It’s control. 🕵️♀️💉
Mike P
Let me tell you something, folks. We’ve got the best damn medical system in the world. And if you think we need more gloves and robots to handle chemo, you’re not seeing the big picture.
China’s got AI doing surgeries. Russia’s got nuclear-grade containment. And here we are, arguing over whether a nurse should wear two gloves or three.
Real talk - if you can’t handle chemo in the U.S., go work in a third-world clinic. No CSTDs. No ventilation. No paperwork. Just a syringe and a prayer. Bet you’ll shut up then.
And home chemo? You think Americans can’t follow instructions? We can. We just need a little discipline. No one’s handing out pamphlets because we’re lazy - we’re giving people responsibility. That’s what freedom looks like.
Stop whining. Start training. And if you’re scared? Don’t touch it. But don’t make the rest of us pay for your fear.
Keith Helm
The implementation of closed-system transfer devices is an essential component of occupational health infrastructure. The permeation thresholds established by NIOSH and USP are non-negotiable. Failure to comply constitutes a violation of 29 CFR 1910.1200. The economic analysis presented is insufficiently granular. Capital expenditure should be amortized over the expected service life of equipment, not evaluated as a one-time cost.
Furthermore, the integration of AI-based verification systems must adhere to FDA 21 CFR Part 11 for electronic records. Without validation protocols, the proposed solution introduces systemic risk.
Recommendation: Engage a certified industrial hygienist to conduct a risk assessment prior to procurement.
Jasmine Bryant
Wait - so if you’re mixing chemo and your glove tears after 25 minutes, you’re supposed to change it? But what if you’re in the middle of preparing 5 bags and no one’s there to help? Do you just stop and wait? That’s not safe either.
I think the rules are right, but the system’s broken. We need more staff, not more steps. And why aren’t we training caregivers the same way we train nurses? My mom’s chemo bag leaked and she didn’t know what to do. They didn’t even give her a spill kit.
Also - is the AI thing real? Or is it just a buzzword? I saw a video where the scanner beeped at a bottle that was labeled right. So… what’s the point?
Also, I think I misread ‘P100’ as ‘P10’ at first. Oops. 😅
shivani acharya
Okay, so let me get this straight - we’re spending $35k on a machine that stops drugs from leaking… but the same hospital can’t afford to hire a second nurse to help with the fourth check? And we’re supposed to believe this is about safety?
Let’s be real. This isn’t about protecting nurses. It’s about protecting hospitals from lawsuits. They want you to think the gloves are the hero. But the real hero? The nurse who works 12 hours straight, gets no breaks, and still remembers every patient’s name.
And the ‘24/7 hotline’? Please. I’ve called those. They transfer you three times, then tell you to ‘call back during business hours.’
And the ‘color-coded bags’? I’ve seen them. They’re the same color as the trash bags they use for diapers. No one takes them seriously.
They’re throwing glitter on a sinking ship and calling it innovation.
And don’t even get me started on the ‘living document’ nonsense. If it changes every 5 years, that means they’ve been lying for the last 20.
They’re not fixing the system. They’re just making it more complicated so they can charge more.
And the worst part? We all know it. But we’re too tired to fight.
So we just keep putting on the gloves. And hoping.
That’s not safety. That’s survival.
Ryan Riesterer
Current exposure thresholds for dermal absorption of alkylating agents (e.g., carmustine) exceed permissible limits under NIOSH REL-2023 when single-glove protocols are employed. CSTDs reduce airborne particulate concentration by 92–98% in non-ventilated environments, per ESMO 2023 meta-analysis. The fourth verification protocol reduces misidentification errors by 18.3% (NCCN 2022), with a 95% CI of ±2.1%.
Home chemo incident rates remain elevated due to inadequate PPE dissemination, not patient noncompliance. The ASCO toolkit demonstrates a 41% reduction in caregiver-reported anxiety (p<0.01).
AI verification systems reduce procedural latency by 14% while increasing compliance fidelity. Implementation requires integration with HL7 FHIR standards for interoperability.
Recommendation: Prioritize CSTD deployment in facilities with >20 chemo administrations/week. Cost-benefit analysis yields ROI within 14 months.
Brenda King
I just want to say thank you to every nurse who’s ever worn those double gloves.
I’ve seen it. I’ve been there. I’ve held my mom’s hand while she cried because she didn’t want to be a burden.
And I’ve watched the nurse who gave her the drug - tired, quiet, but still checking the name twice. Still changing gloves. Still wiping the table. Still smiling.
That’s not protocol. That’s love.
And if we can’t afford to give you the tools to do that safely? Then we’re not just failing you.
We’re failing them.
So please - keep going.
We see you.
And we’re so sorry it’s this hard.
❤️
Liberty C
How is it possible that in 2024, we’re still having this conversation? We have CRISPR, self-driving cars, and AI-generated poetry - but we can’t ensure nurses don’t get cancer from their own job?
It’s not incompetence. It’s greed. Hospitals are for-profit entities. Safety is a line item. Nurses are expendable. Patients are revenue streams.
The ‘fourth verification’? A PR stunt. The CSTDs? A tax write-off. The ‘living document’? A way to delay accountability.
And the ‘home chemo toolkit’? A Band-Aid on a severed artery.
This isn’t a medical issue. It’s a moral failure dressed in lab coats.
And you? You’re still reading this, thinking it’s just another article.
But one day, it’ll be your mother. Or your sister. Or you.
And then you’ll remember this post.
And you’ll be furious.
Good. You should be.
Neil Ellis
Man, I just read the part about the gloves transferring to your phone. That’s wild. I bet half the nurses have chemo residue on their AirPods.
And the fact that you can’t take your gown home? I’d probably try. Just to save laundry money. 😅
But seriously - if your phone’s contaminated, maybe we need a ‘Chemo-Free Zone’ policy. No phones in the med room. Like a no-phone zone in the hospital cafeteria, but for poison.
Also - who’s cleaning the spill kits? Are they getting paid extra for that? I bet not.
Just saying. We’re asking people to risk their health, but not paying them enough to afford a second car seat for their kid. That’s messed up.
Margaret Khaemba
Yeah. That’s the quiet part. No one gets hazard pay for handling chemo. No one gets hazard leave when they get infertility. No one gets therapy after they find out their gloves failed and they’re now at higher risk for leukemia.
And the worst part? We don’t even talk about it. We just keep showing up.
That’s not courage. That’s capitalism.